Abstract
Significant improvements in human rights and democracy have been made since the adoption of the Universal Declaration of Human Rights by the United Nations in 1948. Yet, human rights, especially women’s rights, are still being violated in many parts of the developing world. The adverse effects of such violations on women’s and children’s health are well known, but they are rarely measured. This study uses cross-national data from over 145 countries to estimate the impact of democracy and respect for human rights on various measures of women’s health while controlling for confounding socio-economic factors such as income, education, fertility and healthcare. It finds that democracy and regards for human rights contribute positively to women’s health outcomes, as do socio-economic variables.
Keywords: Democracy, Human rights, Mortality rates, Socioeconomic determinants of health, Women’s health
Introduction
Every year December 10 is marked worldwide as Human Rights Day in commemoration of the United Nations Universal Declaration of Human Rights adopted on the same day in 1948. Since then, significant progress has been made in recognition, respect and promotion of human rights in many parts of the world. At the same time, however, other parts of the world have either seen no progress in this regard or, worse yet, experienced a deterioration of human rights and conditions.
Despite some advances in gender equality over the past several decades, women have taken the brunt of human rights violations and endured disproportional suffering as a result. They have paid dearly with their health and their lives. The heavy toll on women’s health and well-being is mostly attributed to their unique vulnerabilities which include, among other things, risks of sexual exploitation and violence (UNICEF, 2003[13]; WHO, 2005[16]; Sen et al.,2006[11]; Gross et al.,2006[5]; Naved et al.,2006[8]; Dasgupta, 2007[3]; Castro et al.,2008[1]); reproductive health risks (WHO, 2004[15]; Mathers and Loncar, 2005[7]); child rearing and domestic work; discriminatory socio-cultural practices and attitudes toward women; and economic dependency and poverty in many parts of the developing world (Pogge, 2005[9]; Sen et al.,2006[11]; Singh and Singh, 2008[12]; Safaei, 2009[10]).
To get a sense of the magnitude of women’s ill-health and suffering worldwide, the WHO’s Report on Women and Health (WHO, 2009[17]) indicates that, as late as 2008, about 1000 women died every day due to complications of pregnancy and child birth, including severe bleeding, after delivery, infections, hypertensive disorders, and unsafe abortions. Of the 1000 deaths, 570 were in Sub-Saharan Africa, 300 in South Asia and only five in high-income countries. As well, every year some 9 million children under 5 years, including 4.3 million girls, die mainly due to low-birth weight, neonatal infections, diarrhea-related diseases and pneumonia with a vast majority of it being neonatal deaths (WHO, 2009,[17] p.19).
It is now well known that morbidity and mortality are deeply rooted in the socio-economic conditions in which people live and work. What is often ignored is the fact that socio-economic conditions are very much defined by the political structures that frame those socio-economic conditions. Moreover, the political environment and institutions directly interact with human conditions through respecting or violating human rights, promoting or repressing political freedoms and civil liberties, encouraging or discouraging civic engagement and self-determination, and creating or preventing an environment of hope and optimism for the future. Given the above-mentioned vulnerabilities and the historical evidence, women stand a much larger chance to gain from democracy and respect for human rights and lose from dictatorship and neglect of human rights.
In an earlier study (Safaei, 2009[10]) the direct and indirect effects of democracy and respect for human rights on women’s health were outlined using a conceptual model. The present study complements the former by providing empirical evidence on the links between democracy and human rights on women’s and children’ health while controlling for other confounding factors such as income, education, fertility and expenditure on healthcare using a large sample of countries around the world.
The rest of the paper is organized as follows. Section II describes the empirical model along with measures of women’s health, socio-economic indicators and indices of democracy and human rights. Section III provides summary data and estimation results and discusses the empirical findings. And section IV concludes the paper.
The Empirical Model
The general regression model linking a health outcome to determinants of health is specified as follows:
Health = f (Income, Education, Fertility, Healthcare, Democracy/Human Rights)
The health outcomes considered in this study are maternal mortality rate per 100,000 live births (MMR), female adult mortality rate per 1000 population (AMR) and female life expectancy at birth in years (LEB). As well, still birth rate (SBR), neonatal mortality rate (NMR), infant mortality rate (IMR) and child mortality rate (CMR) – all per 1000 live births – are considered. The latter mortality rates are either directly related to mothers’ health or closely associated with mothers’ health and well-being. All the health data are taken from the WHO Global Health Observatory database (GHO, 2011[18]). The most recent data for MMR are those for 2008, for AMR, LEB and SBR are those for 2009, and the rest are those for 2010.
The socio-economic determinants considered are gross national product per capita in log form (GNP) to serve as a measure of average income or material well-being, female adult literacy rate (LIT) as a measure of education, the fertility rate (FRT) as a demographic factor which has significant implications for mothers’ and children’s health, and social security health expenditure as a proportion of total government health expenditure (SSH) considered as a proxy for access to healthcare services. The data on GNP and SSH are for 2008 and taken from WHO (GHO, 2011[18]). The fertility data are for 2009 and obtained from the World Bank Data (World Bank, 2011[19]). The literacy rates are the latest available data belonging to the time period 2005-2009. The latter are taken from the United Nations Statistical Division (UNSD, 2011[14]).
Two sets of political variables are used to capture democracy and human rights. The first set consists of two dummy variables that identify free and partially free countries as classified by the Freedom House political rankings for 2010 (Freedom House, 2011[4]). The variables are labelled as FREE and PFREE, respectively. The second set includes Governance Scores on Rule of Law (labelled as ROLA) as measured by the Worldwide Governance Indicators for 2009 (WGI, 2010[6]). These continuous scores range from -2.5 to +2.5 with higher scores indicating greater observance of rules and democracy. There are a number of indices of human rights defined and measured by the Cingeranelli – Richards (CIRI) Human Rights Dataset (CIRI, 2011[2]) some of which are focussed on women’s rights. However, these indices are categorical and could not be used along with other continuous data. The estimation results, which are based on observations from 141 to 146 countries, are reported and discussed in the following section.
Estimation Results
Before getting to the estimation results, a summary of the sample data for various measures of health and socio-economic variables would be helpful. Such data are reported in Tables 1 and 2, respectively.
Table 1.
Summary data for health measures
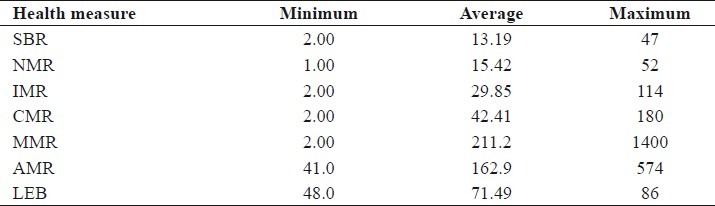
Table 2.
Summary data for health determinants
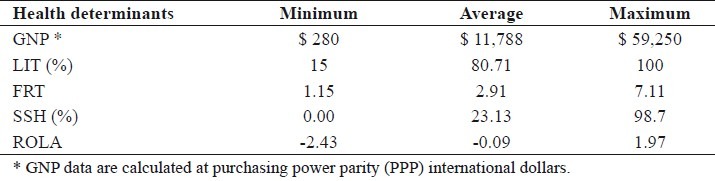
As the above tables show, there are wide variations in both health measures and health determinants across the sample countries. The study draws upon such cross country variations to estimate the empirical model relating various health outcomes to health determinants.
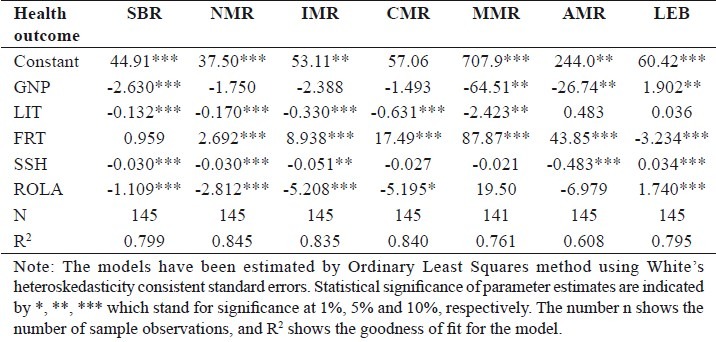
The empirical model is estimated for each of the seven measures of health described above using the socio-economic and political determinants. Two sets of results are reported. The first set, which is given in Table 3, corresponds to the polity dummy variables that identify free and partially free countries. The second set, which is provided in Table 4, is related to the continuous governance scores as a measure of democracy and human rights.
Table 3.
Estimation results with dummy polity variables
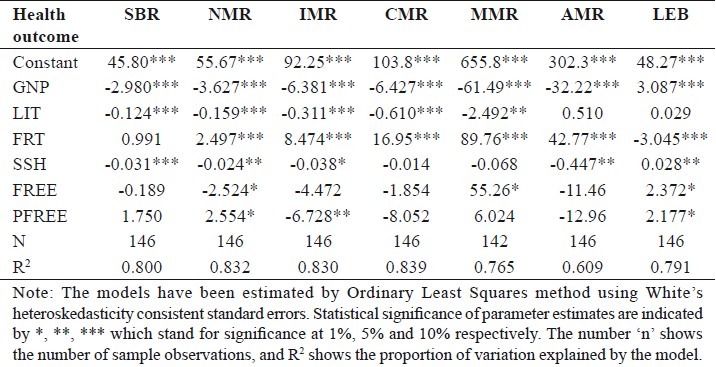
Table 4.
Estimation results with governance scores
The findings in Table 3 show that a country’s average income (GNP) is strongly related to health outcomes. It is negatively related to mortality rates and positively related to LEB. Such favorable impact of income on health outcomes is statistically highly significant. In terms of the magnitude of the effects, a unit increase in log of GNP (amounting to roughly $5100 increase in per capita income around the sample mean) reduces IMR by 6.4 (per 1000 live births) and MMR by 61.5 (per 1000 live births), while increasing LEB by over 3 years. Also, female adult literacy rate (LIT) has a statistically significant positive impact on all health outcomes, except for female AMR and LEB. Higher literacy rates are associated with lower mortality rates among children. A 10 percent increase in the literacy rate reduces IMR by 3 and CMR by 6, for example. Fertility rate (FRT) also shows strong and statistically significant relationships with health outcomes. It is positively related to mortality rates and negatively to life expectancy. For example, a unit increase in the average fertility rate in a country is associated with 2.5 increase in neonatal mortality (NMR), 8.5 increase in IMR, almost 17 increase in CMR, or an increase of 90 in MMR but a decrease of 3 years in female LEB. SSH is also negatively related with mortality rates and positively related to life expectancy, although not significantly as other variables. The polity variables (FREE and PFREE) generally follow the same pattern of being negatively related to mortality rates and positively to LEB. However, their parameter estimates are either not statistically significant or significant at 10%. The exception is IMR where the parameter estimate for free countries is significant at 5% indicating that, controlling for other things, free countries have a lower IMR by 6.7 (per 1000 live births).
Turning to the findings in Table 4, it can be seen that income (GNP) is still favorably related to health outcomes, although some relationships (e.g., with NMR, IMR and CMR) are not statistically significant. The magnitudes of the parameters are comparable to those reported in Table 3. Literacy (LIT) maintains the same pattern of association with health outcomes as in Table 3, negatively related to children and maternal mortality rates, but not to AMR and LEB. As well, fertility shows the same pattern of impacts on mortality rates and life expectancy. Such effects are highly statistically significant with same order of magnitudes as in Table 3. SSH shows stronger associations here with 5 out of 7 parameters being statistically significant at 5% or less. The magnitudes of the parameters are rather small, however. Finally, the governance score (ROLA) that captures state of democracy and human rights in a country, shows statistically significant relationships with most of the health outcomes that are of the expected signs. Higher scores on the Rule of Law are associated with lower mortality rates (except for MMR and AMR) and higher LEB. For example, a unit increase in ROLS score reduces CMR by more than 5 and increases LEB 1.7 years.
Concluding Remarks [See also Figure 1: Flowchart of Paper]
Figure 1.
Flowchart of the paper
The empirical findings as reported in Tables 3 and 4 clearly show that the socio-economic variables income and education are key determinants of women’s and children’s health. In addition, they show that fertility rate is a major determinant of health, which is statistically highly significant in all the models. Although fertility rate is conventionally considered as a demographic variable, it is actually a barometer of cultural norms, deeper gender power structure and availability of basic resources for birth control. In other words, it reflects a conflation of socio-economic and political circumstances that define women’s reproductive rights. Access to effective healthcare is an important factor for women’s and children’s health, especially in developing countries where no universal healthcare insurance is available. As a result, public coverage of health care for the vulnerable (mainly women and children) must improve their access to healthcare. The findings support the favorable effect of such protection on women’s and children’s health.
Given the sizable positive correlations between socio-economic determinants and polity variables, it is often hard to disentangle the separate or direct effect of polity on health. Nevertheless, the findings in this study do provide evidence for the direct influence of polity on women’s and children’s health. Such evidence is more pronounced for the continuous governance scores than the categorical polity variables. Aggregate cross-national analysis subdues within country variations which may be enormous; however, it provides a sharper global picture.
Take home message
Socio-economic and political factors are very important for the health of populations.
Democracies make substantial contribution to women’s and children’s health by way of improving their socio-economic conditions and respecting their human rights.
Developing countries must democratise and promote human rights along with their economic development to narrow their health divide with the developed countries.
Questions that this Paper Raises
What are the broader determinants of health and well-being?
What are the health risks to which women are uniquely exposed?
How might we reduce or eliminate women’s health risks?
How does respect for human rights affect women’s health?
What is the role of culture in shaping demographic patterns?
How are socio-economic and political determinants of women’s health related?
About the Author
Jalil Safaei, PhD, is an associate professor of economics at the University of Northern British Columbia in Canada. He was an affiliate with the Center for Health Services and Policy Research at the University of British Columbia, and is currently a fellow of the Royal Society for Public Health in United Kingdom. His areas of interest include politics of health, social determinants of health and health inequality, macroeconomics of health, and economic evaluation of health care services and policies.
Acknowledgment
I would like to thank the MSM editors and Dr. A.R. Singh for the invitation for this contribution.
Footnotes
Conflict of interest: None declared
Declaration
This is my original, unpublished work, not submitted for publication elsewhere.
CITATION: Safaei J. Democracy, Human Rights and Women’s Health. Mens Sana Monogr 2012; 10: 134-42
References
- 1.Castro R, Casique I, Brindis CD. Empowerment and Physical Violence Throughout Women’s Reproductive Life in Mexico. Violence Against Women. 2008;14:655–77. doi: 10.1177/1077801208319102. [DOI] [PubMed] [Google Scholar]
- 2.The Cingranelli- Richards (CIRI) Human Rights Database. 2011. [Last accessed 2011 Dec 10]. Available from: http://www.cirri.binghampton.edu .
- 3.Dasgupta SD, editor. Body Evidence: Intimate Violence Against South Asian Women in America. New Brunswick, NJ: Rutgers University Press; 2007. [Google Scholar]
- 4.Freedom House. 2011. [Last accessed on 2011 Nov 30]. Available from: http://www.freedomhouse.org .
- 5.Gross AM, Winslett A, Roberts M, Gohm CL. An Examination of Sexual Violence Against College Women. Violence Against Women. 2006;2:288–300. doi: 10.1177/1077801205277358. [DOI] [PubMed] [Google Scholar]
- 6.The Worldwide Governance Indicators. 2011. [Last accessed on 2011 Nov 30]. Available from: http://info.worldbank.org/governance/wgi/index.asp .
- 7.Mathers CD, Loncar D. Updated projections of global mortality and disease: 2002-2030. Data sources, methods and results. Geneva: World Health Organization, Evidence and Information for Policy Working Paper; 2005. [Last accessed on 2011 Nov 21]. Available from: http://www.who.int/healthinfo/statistics/bodprojectionspaper.pdf . [Google Scholar]
- 8.Naved RT, Azim S, Bhuiya A, Persson LA. Physical Violence by Husbands: Magnitude, disclosure and help-seeking behaviour of women in Bangladesh. Soc Sci Med. 2006;62:2917–29. doi: 10.1016/j.socscimed.2005.12.001. [DOI] [PubMed] [Google Scholar]
- 9.Pogge T. World Poverty and Human Rights. Ethics & International Affairs. 2005;19:1–7. [Google Scholar]
- 10.Safaei J. Democracy and Women’s Health. Mens Sana Monogr. 2009;7:20–36. doi: 10.4103/0973-1229.42101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sen G, Östlin P, George A. Geneva: WHO; 2006. [Last accessed on 2011 Nov 15]. Unequal, unfair, ineffective and inefficient – Gender inequity in health: why it exists and how we can change it. Available from: http://www.who.int/social_determinants/resources/csdh_media/wgekn_final_report_07.pdf . [Google Scholar]
- 12.Singh AR, Singh SA. Diseases of Poverty and Lifestyle, Well-Being and Human Development. Mens Sana Monogr. 2008;6:187–225. doi: 10.4103/0973-1229.40567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.UNICEF. United Nations High Commissioner for Refugees. Sexual and Gender-Based Violence against Refugees, Returnees and Internally displaced Persons – Guidelines for Prevention and Response. United Nations High Commissioner for Refugees. 2003. [Last accessed on 2011 Nov 15]. Available from: http://www.unicef.org/violencestudy/pdf/UNHCR%20-%20SGBV.pdf .
- 14.United Nations Statistical Division, UNSD Statistical Databases. 2011. [Last accessed on 2011 Dec 1]. Available from: http://www.unstats.un.org/unsd/databases.htm .
- 15.Maternal mortality in 2000: estimates by WHO, UNICEF and UNFPA. Geneva: World Health Organization; 2004. WHO. [Google Scholar]
- 16.Multi-country Study on Women’s Health and Domestic Violence against Women – initial results on prevalence, health outcomes and women’s responses. Geneva: World Health Organization; 2005. WHO. [Google Scholar]
- 17.Report on Women and Health: Today’s Evidence Tomorrow’s Agenda. Geneva: World Health Organization; 2009. [Last accessed on 2011 Nov 28]. WHO. Available from: http://www.who.int/gho/women_and_health/en/index.html . [Google Scholar]
- 18.Global Health Observatory. 2011. [Last accessed on 2011 Nov 25]. Available from: http://www.who.int/gho/en/
- 19.The World Bank Data. 2011. [Last accessed on 2011 Nov 25]. Available from: http://data.worldbank.org/indicator .