Abstract
This paper highlights the mental health needs of the elderly. It tackles the issues of their institutionalisation and community care. Rapid urbanisation in Indian society throws up special problems in elderly care. There is great evidence of a raise in morbidity, mortality, hospitalisation and loss of functional status related to common mental disorders in the elderly patients. Overlap of depression and anxiety is very common with up to almost half of the elderly patients reporting significant depressive and anxiety symptoms. Also, depression is the most common psychiatric disorder in late life. Growth in the elderly population means a direct increase in age related diseases such as dementia and poor mental health outcomes such as depression, anxiety, suicide and serious constraints on the quality of life among elderly individuals.
The need to identify new and unmet problem areas and develop efficient therapeutic outcomes for this special population is stressed.
Keywords: Age-related diseases, Alienation, Ashramas, Institutionalisation and community care, Misconceptions about elderly and ageing, Overlap of depression and anxiety, Pitras, Poor mental health outcomes, Rina, Social isolation, Traditional Indian culture, Urbanisation, Vriddha
Introduction
Old age is a worldwide phenomenon, generally accompanied by a number of problems that the aged have to face and get attuned to. There is a great body of evidence of a rise in morbidity, mortality, hospitalisation and loss of functional status related to common mental disorders in the elderly patients. Overlap of depression and anxiety is very common in older adults, with up to almost half of the elderly patients reporting significant depressive and anxiety symptoms.
As the number of aged in our population is increasing, many of their traditional life sustaining and fostering influences have been eroding. Changes in society seem to leave them no meaningful social role either within the family or in the community. Often, the elderly are socially isolated, and many exist within the confines of a nursing home or an institution, where their main social links are only with other inmates and equally alienated old people.
Greco-Roman and American Cultures Views on Aged and Ageing
In Greek and Roman cultures, 80% of the population perished before reaching the stage of life commonly identified as middle age today. For Aeschylus, age brought with it wisdom, especially about justice and prudence. Although Aeschylus refers to the negative experience of age, mainly loss of physical strength, he insists that physical decline has no impact on the older person’s mind or spirit. In contrast, Sophocles portrays old age as distasteful, as a time of deterioration in physical and mental functioning.
In 17th and 18th century America, old age was considered with respect, as it was so rare. Old men occupied the highest public offices, as well as positions of authority within the family until they died; fathers waited until their sixties before giving their land to their eldest son. Church seats were given to the old. The primary basis of the power enjoyed by the elderly in colonial times was their control of the property, especially productive property in farmland. In such an agricultural society, such control amounted to the ability to dominate all key institutions – the family, the church, the economy and the polity.
Traditional Indian View of Life and Ageing
In most gerontological literature, people above 60 years of age are considered as ‘old’ and as constituting the ‘elderly’ segment of the population. In traditional Indian culture, a human life-span is 100 years. Manu, the ancient lawgiver, in his Dharmashastra divided this span of life into four ‘ashramas’ or life stages. The first, ‘brahmacharya’ (life of a student) was to be spent at the teacher’s (guru’s) house. This is the life of a celibate, to be exhausted in education and training. Once the education was complete, the boy (grown into adulthood by now) would be ready to enter the ‘grihastha ashram’, the life of a householder. This was the stage when a man would fulfil his basic desires, for love, marriage, for parenthood, for status, wealth, prestige and other such physical and social needs. He was to discharge the debts he owed to the parents and ancestors (pitr-rina) by begetting sons and to the gods (deva-rina) by performing Yajnas (rituals). When a man’s noteworthy head turned grey and wrinkles appeared, he was to give up this life of a householder and turn to ‘vanaprastha’ by which an older and ageing man would steadily give up worldly pursuits, move away from the ordinary routine of the householder and spend life in search of spiritual growth. Finally, when he was spiritually ready, he would renounce the world completely and enter the stage of ‘sanyasa’ or ‘asceticism’.
In Indian literature, the aged is generally termed the “Vriddha” (advanced). Four types of vriddhas are described in ancient Indian literature:
Tapo-vraddha: Who is advanced in penance.
Kala-vraddha: Who is advanced in age.
Jnana-vraddha: Who is advanced in knowledge; and
Dhana-vraddha: Who is advanced in wealth.
The old are respected in India as parents or ‘pitras’. The Upanishads advise people to respect the father, the mother, the teacher, and the guest as God. In the Ramayana and the Mahabharata, the two great epics of India, there are many lively and moving episodes showing the reverence of the young for the old. Even today, in India, old parents live with son/s and their families. Living with the eldest son and his family is the most familiar phenomenon. This tradition ensures that old people have younger in-laws and grandchildren to care for them. Furthermore, caste and kin groups exert pressure on younger members to obey and respect elders.
In modern India, retirement age is fixed at 58 in most Government jobs, and 60 years in the Universities. However, middle-class Indians are strongly oriented towards maintaining their autonomy. The parents are much more prepared to invest their money and efforts on children in India than is the norm in many western countries. It is taken as a normal duty of the sons to take care of the needs of the parents. Thus, social dependency is a common feature of India.
Misconceptions about Older People and Institutional Care
There are always some misconceptions about older people and the ageing process. As a product of a youth-oriented society, we have all learned negative attitudes about ageing; therefore, older people may encounter many stereotypes and myths. However, despite philosophical attitudes and cultural values, surveys carried out by different people have shown that depression is the most common psychiatric disorder in late life.
In last few decades, the debate on issues like institutionalisation and community care has gained considerable importance. The increased demand for alternative care for the elderly, however, raises a million-dollar question: the formal care systems are insufficient in terms of quality of care and also in quantitative capability. This is reflected more in low-income countries, e.g., in China 12 million elderly people are in need of assistance in their day to day life while only 0.05% are accommodated in institutional care. In contrast, in high-income countries, 4-6% of elderly are in some sort of institutional care. Nevertheless, there are greater differences in provision and/or acceptance of institutional care in many countries due to factors like culture, economy, environment and demography. It is not yet apparent whether social changes like increasing urbanisation, breakdown of the joint family system, women getting more career-oriented, will compel even traditional societies to follow the institutionalisation system for the elderly. However, such a kind of consideration in health care policy and/or social policy cannot be ruled out at this point. The moot point is: are these services efficient to maintain psychological well-being in the elderly?
It is observed that the provision for general health care in institutional inmates was poor or even absent at times. Mental health care facility was conspicuously absent in the programme for care of the elderly in these institutions. For them, basic needs like eating and shelter were more important than quality care in terms of health. The elderly appeared to be lonely and dejected. The worthlessness and demoralisation were quite obvious in these institutions. The elderly in the community enjoyed better social support than those in the institution. Perception of self-esteem and psychological well-being is expected to be better in a community population. Compared with this, covert depression was found to be more in the institutionalised elderly. It should be noted that community care provides elderly population more of social integration and diminishes the feeling of loneliness and rejection. Of course being with the family does not guarantee emotional as well as social security, as there are many case reports of elderly abuse and exploitation coming in from the community.
Age-Related Diseases
Thus, old age brings with itself lots of problems. With the increase in the elderly population, health status of the elderly has gained lots of importance. However, neither institutional nor community care has provided an adequate solution to the problems of old age. Though community care is preferred over institutionalisation, lack of funding acts as a major hindrance. Hence, the need of the hour is to integrate the services provided by institutions as well as community to improve the quality of life of the elderly population. More research is needed to develop acceptable models of care to meet the facilities for long-term care, and that includes institutionalisation. We still need to learn about efficient models of formal care systems in traditional societies like India and their cost effectivity, and then decide about informal care system with same perspective, as cultural adaptation is essential for the elderly to feel good and be healthy.
Growth in the elderly population means a direct increase in age-related diseases such as dementia and poor mental health outcomes such as depression, anxiety, suicide and serious constraints on the quality of life among elderly individuals. In India as well, due to the demographic transition, rapid industrialisation and urbanisation, westernisation of Indian culture and disintegration of joint or extended family structures into nuclear ones, the susceptibility of the older population has increased. They have become exposed not only to their physical disabilities but also to social, economic and emotional alienation and isolation. An associated social change with industrialisation has led to changes in the routine of the elderly, resulting in reduced social participation, loss of dignity and self-respect. Eventually, it weakens the social and family support of an individual resulting in declining mental health.
With the breakdown in the traditional joint family structure, where both young and old were absorbed with mutual harmony, Indian family structure is steadily undergoing the process of disintegration and nuclearisation. In addition, the elderly are not given the same respect, attention and care they used to get earlier. The above change may be due to limited assets and growth of ‘individualism’ in modern life. Thus, all these aspects lead to isolation of the elderly from family and social life. Even though elders feel capable of working and contributing to family resources, there are no outlets to absorb them.
Hence, ageing can be considered as mainly a social problem leading to decline of mental health because of two factors:
Ageing is a direct problem for the segment of the population which is in that age category. The elderly suffer all consequences — physical and emotional — due to real or perceived alienation from family and society.
It is a social problem for the society as a whole because of the presence of old people, and their problems have profound effects upon the structure, functions and economy of the society.
Thus ageing has brought with it several physical as well as mental problems. For example, older persons use general physician services slightly more than the young. However, in contrast, mental health services, though limited, are drastically under-utilized by the elderly. Modernisation of family structure and economical stressors has threatened the security of the aged in society. More and more aged are on the threshold of becoming homeless without effective infrastructure in the community other than the family.
Institutional Care
Thus, the need for institutional care cannot be underestimated. Institutionalisation is a last resort in cases of severe dependencies, and more and more families are becoming increasingly insufficient to care for a progressively more ill geriatric population. It is happening and will continue to happen as a result of economic, social and cultural issues as well as health care burden. In fact, the conclusion from studies suggests that being elderly and not having a social support set-up are key predictors of institutionalisation rather than health-related and socio-economic variables.
However, the knowledge of psychiatric problems at the institutional level requires to be tackled with utmost care. Multidisciplinary approach with mental health profession as an important element in the intervention of the psychopathological problem is the need of the hour. Institutionalisation is here to stay in our society. We need to improvise the needs, merits and an interventional perspective beyond psychopathology. The issue is not just prevention of a problem, but also promotion of general health, and mental health is an essential aspect of care of the aged. Hence, perspective on quality of life, subjective well-being and emotional support are key concerns for the elderly in the modern era, irrespective of scientific advances in medical care.
Conclusions [Figure 1: Flowchart of the Paper]
Figure 1.
Flowchart of the paper
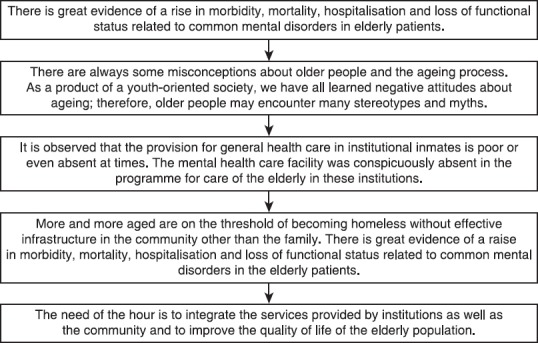
There is great evidence of a rise in morbidity, mortality, hospitalisation and loss of functional status related with common mental disorders in elderly patients As the number of aged in our population is increasing, many of the traditional life sustaining and fostering influences for the elderly have been eroding. Changes in society seem to leave the aged no meaningful social role either within the family or in the community.
In Indian literature, the aged are generally termed “Vriddha” (advanced). Four types of vriddhas are described in ancient Indian literature:
Tapo-vraddha: Who is advanced in penance.
Kala-vraddha: Who is advanced in age.
Jnana-vraddha: Who is advanced in knowledge; and
Dhana-vraddha: Who is advanced in wealth.
There are always some misconceptions about older people and the ageing process. As a product of a youth-oriented society, we have all learned negative attitudes about ageing; therefore, older people may encounter many stereotypes and myths.
In last few decades the debate on issues like institutionalisation and community care has gained considerable importance. The increased demand for alternative care for the elderly, however, raises a million-dollar question: The formal care systems are insufficient in terms of quality of care and also in quantitative capability. It is observed that the provision for general health care in institutional inmates is poor or even absent at times. The mental health care facility was conspicuously absent in the programme for care in the elderly in these institutions.
Growth in the elderly population means a direct increase in age-related diseases such as dementia and poor mental health outcomes such as depression, anxiety, suicide and serious constraints on the quality of life among elderly individuals. In India as well, due to the demographic transition, rapid industrialisation and urbanisation, westernisation of Indian culture and disintegration of joint or extended family structures into nuclear ones, the susceptibility of the older population has increased.
Ageing has brought with it several physical as well as mental problems. For example, older persons use general physician services slightly more than the young. However, in contrast, mental health services, though limited, are drastically under-utilized by the elderly. Modernisation of family structure and economical stressors has threatened the security of the aged in society. More and more aged are on the threshold of becoming homeless without effective infrastructure in the community other than the family. There is great evidence of a raise in morbidity, mortality, hospitalisation and loss of functional status related to common mental disorders in the elderly patients.
The need of the hour is to integrate the services provided by institutions as well as community to improve the quality of life of the elderly population. More research is needed to develop acceptable models of care to meet the facilities for long-term care, and that includes institutionalisation. We still need to learn about efficient models of formal care systems in traditional societies like India and their cost effectivity, and then decide about informal care system with the same perspective, as cultural adaptation is essential for elderly to feel good and be healthy.
Take Home Message
Ageing has brought with it several physical as well as mental problems.
Older persons use general physician services slightly more than the young. However, in contrast, mental health services, though limited, are drastically under-utilized by the elderly.
Modernization of family structure and economical stressors threaten the security of the aged in society. More and more aged are on the threshold of becoming homeless without effective infrastructure in the community other than the family.
We need to integrate the services provided by institutions as well as the community and to improve the quality of life of the elderly population.
Questions that this Paper Raises
What concrete programmes can work for the mental health needs of the elderly?
What are the problems peculiar to India in this field?
What are those aspects of the needs of the elderly that are common to all societies?
What is the current evidence for institutional and community based help in the elderly, and which is suitable for which elderly group?
About the Author

Shubhangi R. Parkar MD, DPM, MSc, PhD, is Professor and Head, Dept of Psychiatry, G.S. Medical College and KEM Hospital, Mumbai, India. She has also been Ex Dean Incharge at the same institution. She is Chief, Bombay Drug Deaddiction Center, G.S. Medical College and KEM Hospital, Parel. She has been President BPS and IPS West Zone. Her areas of special interest are women’s mental health and suicide.
Footnotes
Conflict of interest
None declared.
Declaration
This is my original unpublished work, not submitted for publication elsewhere.
CITATION: Parkar SR. Elderly mental health: Needs. Mens Sana Monogr 2015;13:91-99.
Peer reviewer for this paper: Anon